
Obstructive Sleep Apnoea
What is Obstructive Sleep Apnoea (OSA)?
Patients with obstructive sleep apnea (OSA) have repeated episodes of partial or complete obstruction of the throat (also known as the "pharynx" or "upper airway") during sleep.
A narrow floppy throat is also more likely to vibrate during sleep, which causes snoring. If partial or complete obstructions occur breathing is reduced or stops for a short time – from 10 seconds up to a minute or more – and blood oxygen levels fall as a result. A brief interruption to sleep (an arousal) that lasts for as little as 3 seconds then occurs, allowing breathing to start again but your sleep is disrupted as a result.
These episodes of obstruction may happen many times – even hundreds of times - overnight.

The risks of undiagnosed OSA include: Heart Attack, Stroke, Irregular Heartbeat, High Blood Pressure, Heart Disease & Decreased Libido. In addition, OSA causes daytime drowsiness that can result in accidents, lost productivity and relationship problems.
What are the symptoms of OSA?
If you have OSA you may snore, toss and turn and others may notice that you stop breathing during the night.
Because of the disruptive effects of OSA on sleep you may find yourself waking up often during the night, sometimes gasping or choking, although this does not always happen.
However, even if there are few awakenings overnight, sleep is disturbed and you may not refreshed due to OSA.
As the day goes on, you may struggle to stay awake, especially in the afternoon. Grumpiness and other mood changes are common in untreated OSA.
How is OSA diagnosed?
Signs and symptoms such as snoring, obesity, observed breathing pauses and sleepiness during the day may suggest that a person has OSA.
The best way to be really sure is with an overnight sleep study. This measures your sleep, breathing and oxygen levels.
Your GP can refer you for a sleep study with support of Medicare if you meet certain screening criteria.
If you don’t meet the Medicare criteria you can still be referred for a sleep study to find out if you are living with this potentially life threatening condition.
What is the best way to manage and treat OSA?
Managing OSA often involves a range of professionals and their opinion on how best manage your unique presentation. These professionals can include:
- General Practitioner (GP)
- Dentist
- Dietitian/Nutritionist
- Exercise Physiologist
- Specialist Sleep/Respiratory Physician
- Specialist Oral and Maxillofacial Surgeon
- Specialist Ear, Nose and Throat Surgeon
There are clear guidelines for managing OSA and the first evidence-based treatments to explore are the non-surgical options as they have minimal risks to the patient.


Oventus O2 Vent ® Optima Oral Appliance
CPAP uses a small, quiet air pump that takes air from the room and delivers it under gentle pressure to a mask that covers your nose. This acts to hold your throat open during the night. You only use CPAP at night in bed. It is very good in controlling the symptoms and the long term effects of sleep apnoea. It stops the snoring and the machine noise is very much quieter than the snoring was. Sometimes it takes a while to become comfortable with the use of CPAP but if it works for you it is still considered the gold standard with next to zero risk. The problem with CPAP is that it is quite commonly not tolerated long term and if you are not wearing for several hours each night, then the treatment will likely not be successful.
A number of other remedies have been marketed to the Australian public, some of which have value for selected patients while many others have been shown to be of no benefit. Your Sleep Physician or Specialist Oral and Maxillofacial Surgeon will be able to advise you. Dr John Webster has an interest in the surgical management of OSA and remains up to date on the latest research and advances in Sleep Medicine to be able to offer patients the spectrum of solutions and works with Sleep and Respiratory Physicians across Toowoomba and the Darling Downs to ensure optimum care for patients with OSA.
What are the surgical treatments of OSA?
There are several surgical operations available for sleep apnoea. These are not usually offered unless both CPAP and oral appliances have not been successful for you. It is important to select the right operation that corresponds to where the obstruction is occurring in the upper airway.
In the paediatric population, the common surgical procedures are focused on the nasal airway, tonsils and adenoid tissues and these treatments are performed by Specialist Ear, Nose and Throat (ENT) Surgeons.
In the adult population the most successful surgical procedure with the highest cure rate is Maxillomandibular Advancement (MMA).
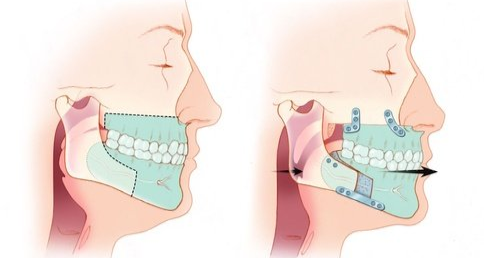
MMA is a procedure performed by Dr John Webster (Specialist Oral and Maxillofacial Surgeons) that surgically moves the upper and lower jaws forward along with the soft tissues of the tongue and palate, opening the upper airway and increasing the tension of the walls so the airway cannot collapse during sleep.
For some patients, the MMA is the only technique that can create the necessary air passageway.

There are some soft tissue procedures such as:
- Uvulopalatopharyngoplasty (UPPP)
- Hyoid Suspension and
- Genioglossus Advancement
that have shown less success and cure rates for OSA however in some cases they remain indicated due to the level of obstruction identified or if a patient has a reason they cannot have an MMA procedure performed.
Historically in the 1980's and 1990's the ‘Standford Protocol’ suggested soft tissue procedures should be undertaken first prior to hard tissue procedures, such as MMA. However, the research of Holty, Boyd and many others has shown that MMA alone is just as successful without the soft tissue surgeries performed prior to it.
The conclusion is that patients should not have to suffer the risks of multiple surgeries when MMA can achieve the optimum outcome in one procedure.
Dr John Webster can discuss with you the latest surgical techniques including 3D planned patient specific custom re-positioning devices to ensure your jaws and airway can be in the optimum position to open your airway and limit the chance of OSA occurring during your sleep.
The health benefits of managing OSA well cannot be ignored and if your Respiratory or Sleep Physician has not discussed the surgical options with you please arrange a referral to Dr John Webster to discuss these life changing treatments with you.
How can you book in for a consultation regarding your OSA?
If you would like to know how we can help you further, or to book a no obligation initial consultation please phone
07 4580 4733 or alternatively request an appointment now online.
Please bring your medical history, current medications, x-rays, scans and sleep study results to this initial consultation as it will assist in determining if you are a candidate for surgical option in managing your OSA. If do not have any x-rays, scans or sleep study results we can assist in arranging this for you at the Oral Facial & Implant Centre. Feel free to call 07 4580 4733 when convenient to you.


